
Mental health and psychosocial support in emergencies: What working in humanitarian settings has taught me about the Covid-19 outbreak in the UK
Rebecca Horn, a freelance international humanitarian worker from Liverpool, working in areas of conflict and disaster around the world, reflects on recent conversations and media coverage on the mental health impact of Covid-19 in the UK:

World Health Organisation guidance on coping with stress during the COVID-19 Pandemic
I have been working as a psychologist for more than 20 years, and since 2003 have been working mainly in humanitarian settings with people affected by conflict, disaster and other emergencies – including the Ebola outbreak in West Africa.
Over the years, the humanitarian community has learned a great deal about how such events affect the mental health and psychosocial well-being of those involved, and what helps them to recover. Recently I have been increasingly struck by the feeling that the lessons which have been so painfully learned in humanitarian settings about what people need in order to cope with and recover from extremely stressful events have not made their way into practice in the UK.
I first noticed this in the response to the Grenfell Tower disaster in June 2017. In humanitarian settings, when a disaster occurs we know that the response should include the participation of the affected community. This did not happen in the response to the Grenfell Tower fire, and over time it seemed from the TV reports I saw that their exclusion from the process contributed to increased distress for those affected.
I see it again in the response from some quarters to the Covid-19 outbreak. The assumption that large proportions of our population will be ‘traumatised’ by the Covid-19 outbreak and the associated lockdown, or that there will be a ‘mental health pandemic’ to accompany the Covid-19 pandemic, just does not fit with what we know about the impact of situations such as this on mental health and psychosocial well-being. This may be the first time that such a situation has occurred in the UK within the lifetime of most of us, but it is not the first time it has happened. The idea that huge proportions of a population - including frontline responders such as healthcare staff – will need specialist mental health support is not in line with evidence from other emergency situations.
Here, I want to apply some of our learning from humanitarian settings about mental health and psychosocial support to the Covid-19 outbreak in the UK context.
How do emergencies like the Covid-19 pandemic affect mental health?

Children Playing Football in an area IMPACTED by conflict
Statistics produced by the World Health Organization, based on studies of a wide range of emergencies, suggest that whilst almost everybody will experience a range of difficult thoughts and feelings (including fear, grief, uncertainty, hopelessness), most people will improve over time without any expert intervention, as long as they have access to their basic needs (safety, information, food etc) and they remain socially connected.
In populations which experienced war or other conflict in the previous 10 years, around 13% of people developed mild forms of distress, 4% developed moderate forms and 5% developed severe disorders. We would not expect the figures to be higher in our current situation.
What helps to protect people in emergencies from developing mental health problems?
There are ways that good psychosocial well-being can be promoted, and mental health problems can be protected against, which do not require any mental health expertise. These are known as the ‘core principles’ of mental health and psychosocial support in emergencies, and they can be integrated into any type of service (e.g. food provision, health care). These are simple and well-established, yet are rarely in evidence in the UK. I have summarised them briefly below.
Core principles of mental health and psychosocial support in emergencies
Human rights and equity: Ensuring that the marginalised and most vulnerable are able to access services
Do no harm: Assessing the potential impact of a response in order to ensure that even if it is not possible to improve the situation, it does not make it worse. This often involves identifying those people, places, events that bring people together (‘connectors’) and those that can cause division and conflict (‘dividers’), then making sure that a service strengthens connectors and minimises dividers[1].
Building on available resources and capacity: Identifying the strengths, resources and capacities within a community and ensuring that any response or service makes use of these. Even in the worst situations, there are people with skills and capacities which can contribute to the response – and engaging this not only results in a response which is more likely to meet the needs of the population, but also increases the sense of self-efficacy and community-efficacy. This contributes to recovery from distressing events[2].
Participation: Ensuring that those whose lives will be affected by decisions made and actions taken play a part in the decision-making process.
Integrated support systems: Stand-alone psychosocial/ mental health services (e.g. a counselling service that people can access if they want support) are not always helpful – for example, because people are reluctant to access them until their distress becomes severe. It is more effective to integrate psychosocial support and mental health provision into services that people already access, such as healthcare or schools. It can also be integrated informally into services such as beauty salons or bars, with staff being trained to have ‘supportive conversations’ with clients.
Multi-layered supports: We know that people will be affected differently by emergencies, based on the internal and external resources available to them. This means that different types of supports and services are required in order to meet the psychosocial and mental needs of a population.
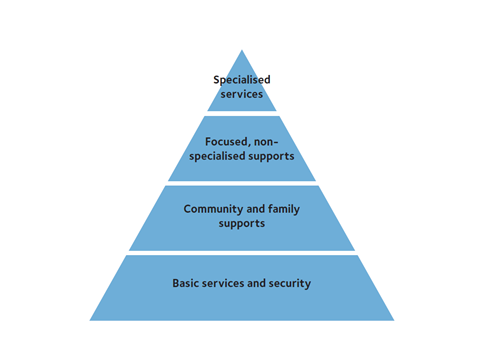
Mental Health and Psychosocial Support Intervention Pyramid
The final core principle is illustrated by the Mental Health and Psychosocial Support Intervention Pyramid[3] (IASC, 2007), which is widely used in emergency contexts.
The pyramid is intended to represent the proportion of a population which will need each type of service in order to maintain good psychosocial well-being and mental health. It shows that everybody affected by an emergency will need basic services and security to be available in a way which is safe, dignified and accessible to people with specific needs. If these services are not available, or are provided in a way which is unpredictable or inappropriate, distress is likely to increase.
A large proportion of the population will need additional supports to ensure that the social connections and networks either remain strong or are rebuilt (if they were disrupted by the emergency). Social connections are essential for good emotional well-being, and promote recovery from distressing events.

MUTUAL SUPPORT IN A CRISIS
As already noted, the majority of a population affected by an emergency will experience painful feelings but will cope and recover over time if these two types of service and supports are in place. A small proportion will experience higher levels of emotional distress which they cannot manage with the normal supports, although they are still able to more or less function in their daily lives. These people can benefit from emotional supports provided by those who are not mental health specialists, but who have been trained and supervised to provide this kind of support to individuals and groups. Then there is a smaller proportion (the 5% with severe mental disorders referred to above) who need specialist mental health care.
What does this mean for supporting the mental health and psychosocial well-being of communities during the Covid-19 outbreak?
The core principles described above were developed for humanitarian settings, and have been applied in many emergencies around the world – including epidemics. People living in the global south are those most often affected by emergencies so our learning about effects on mental health and effective responses mainly comes from those settings, but the current Covid-19 outbreak in the UK is also an emergency and I do not see any reason that our learning would not apply here. Some of the implications of this could be:
Most of us will experience painful emotions during this time. – this is to be expected, and the vast majority will recover without needing any support from mental health professionals.
To promote good psychosocial well-being and mental health (and to prevent mental health problems developing), we all need:
accurate, clear and consistent information, repeated and updated regularly, about the outbreak itself and how we can best take care of ourselves and each other (physically and emotionally)
to be safe
to have access to basic needs (e.g. food, water, shelter, healthcare).
In the UK, many of us are not used to thinking about our access to basic services, we have taken them for granted, but there is a proportion of the population which has never been able to take their access to basic services for granted and is especially at risk now.
Social support is an important element of coping with the outbreak and the lockdown. Many of us are using technology to stay connected with family and friends this, but people who are unable to do this are particularly at risk of becoming more distressed. The barriers to connection may be that a person was isolated even before the outbreak, that they are not familiar with technology, and/ or they do not have access to the technology.
Within small communities and the country as a whole, it would be helpful to identify and strengthen issues, places, people or events that unite us (‘connectors’) and strengthen these. The Thursday evening ‘clap for the NHS’ is one example of this, as was Capt. Tom Moore walking his 100 laps before his 100th birthday. Similarly, it is important to identify and minimise ‘dividers’.
Being involved in the response in some way is likely to be helpful for those who are able to do this. This could include actively participating in local initiatives to support the vulnerable, providing online yoga classes or other activities, even painting a rainbow for your front window to encourage passers-by. The number of people who have signed up to be ‘NHS volunteers’, overwhelming the system, points to the need to be involved in the response. This not only helps others, but also strengthens the volunteer’s sense of self-efficacy – which in itself protects them from higher levels of distress.
Some people just need information and/ or social support in order to reduce their distress, but there will be a small number who need more emotional support. This does not need to be offered by specialists; services like the Samaritans have trained and supervised volunteers who provide this kind of support remotely via phone, Skype, Whatsapp or other means. A proportion of those accessing these services will need specialist mental health care, so should be referred and able to access that.
Ensuring that those with pre-existing mental health problems are able to access the necessary support and medication.
Paying particular attention to the isolated and marginalised, to ensure they are able to receive the services and supports they need. Certain groups of people, including those with pre-existing mental health problems, are particularly at risk when emergencies occur.
What does it mean for supporting healthcare staff and others on the ‘frontline’ of the response?
The MHPSS intervention pyramid is designed to support the coordination of services for affected populations. However, the same principles apply to those who are working on the frontline of the response, who are not only affected by the same anxieties as the rest of the population but are also working long hours in difficult conditions. We can consider the ways in which the MHPSS intervention pyramid might apply to healthcare workers in the Covid-19 response, as outlined below.

The Mental Health and Psychosocial Ssupport intervention pyramid
The two bottom levels of the pyramid are foundational and are required to promote well-being among staff members, and to protect them against stress to some extent (i.e. building resilience). The stronger the bottom two levels are, the fewer staff members will require services at the top two levels of the pyramid.
All healthcare workers involved in the response must have their needs at the ‘basic services and security’ level addressed in order for them to have good psychosocial well-being, and to protect them from developing mental health problems. This would include access to protective equipment and the other materials needed to do their job effectively and safely; adequate pay and compensation; access to food, transport and other necessities. It would normally include adequate rest days and reasonable working hours, but this is unlikely to be possible at this stage in the outbreak. This makes it even more crucial that the other services are in place; if basic needs are not met then levels of distress will increase and a greater proportion of healthcare workers are likely to need emotional support.
Strong relationships both within work teams and with family and friends are also essential; anything that can be done to ensure that responders are able to maintain good, supportive relationships will contribute greatly towards good mental health.
Even with these systems and supports in place, there will be a proportion of healthcare workers who need additional support. For most, this can be provided by people with some training and supervision, but they do not need to be mental health specialists. Ideally, this type of provision would be integrated into healthcare workers’ daily lives rather than being a separate service which healthcare workers have to make efforts to access.
What can we learn from mental health and psychosocial support in emergencies around the world?
The key points to take away from what we have learned from working in humanitarian settings around the world are:
To strengthen psychosocial well-being and promote good mental health, we should focus on providing the basics in a way which strengthens relationships and enables participation.
If we do this, most people will experience painful feelings during the outbreak and immediately afterwards, but will recover without intervention from mental health specialists.
Of those who do need additional support, most will benefit from evidence-based emotional support provided by non-specialists who have been trained and are supervised.
A small number will need specialist mental health services.
Those with pre-existing mental health conditions and those who are isolated or marginalised are most at risk and additional efforts should be made to enable them to get the support they need.
Healthcare workers and others involved in the response are under additional pressures, but the same principles apply.
Originally published on LinkedIn 21st April 2020 - Republished with the author’s permission
Notes:
[1] Anderson, M.B. (1999) Do No Harm London: Lynne Rienner
[2] Hobfoll, S.E. et al (2007). Five essential elements of immediate and mid-term mass trauma intervention: Empirical evidence. Psychiatry, 70 (4) 283-315.
[3] Inter-Agency Standing Committee (2007) IASC Guidelines on Mental Health and Psychosocial Support in Emergencies Geneva: IASC